
Relevant clinical history and physical exam:
Male, 72y.o, retired, was reffered to our hospital as Stabile ungina III CCS. The patient got positive family anamnesis for CAD with previous coronaryprocedures/ PCI/Stenting to mid.RCA and distal RCA due to inferior STEMI/2018/and PCI/Stenting to ostial LAD/also 2018, one month before the present hospitalization. From comorbidities the patient got diabetes/on insulin/. From physical exam with stabile cardiopulmonary status.
Relevant test results prior to catheterization
From non invasive methods:
ECG- SR,HR-78/min,QS III,avF.
Laboratory – referent values of cardiospecific enzymes and other parameters
Echo- referent left chamber diameter, hypokinetic antero-septal and inferior wall. Dyastolic dysfunction. AR I stage.
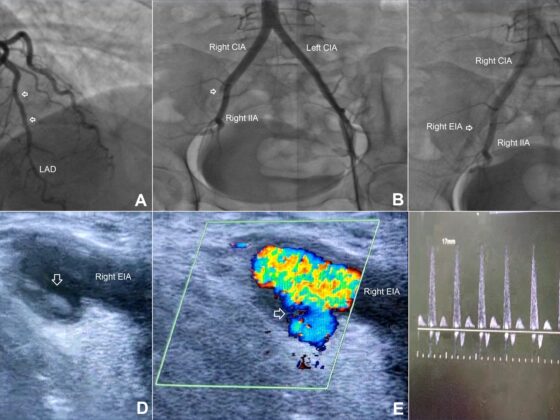
Relevant catheterization findings
Angyo was done through right radial artery/6F indroducer.
From Angyo:
RCA –plaques, stents in m/dRCA-ok.
PL- non-significant stenosis in mid part.
LAD-ost. stent-ok
Stenosis: 40% mLAD, 50% dLAD.
LCx-p/m: plaques, 80% stenosis dLCx after OM2
OM1:60% ostioproximal stenosis
The objective of our treatment was distal LCx.
Coronary
Oktaj Maksudov
BULGARIA
The Houdini Case – Extirpation of stucked ostial LCx stent in the struts of previous implanted ostial LAD stent, ending up with two extirpated stents
[kkstarratings]
You must belogged in to post a comment.